| Other scientists have done some very elegant work associating basic feelings of attachment with elevated activity of oxytocin and vasopressin. |
| The bottom line is that serotonin-enhancing antidepressants that negatively affect this sex drive can quite logically also negatively affect the brain circuits for romantic love. |
| Serotonin-enhancing antidepressants can inhibit other evolutionarily adaptive mechanisms for mate selection. |
| Serotonin-enhancing antidepressants can also inhibit psychologic mechanisms for mate choice. |
| This creates the potential for jeopardizing a patient's personal, social, and genetic future. |
 Here in this article she has wrote about the top 5 regrets that people have on their death bed. All of these are real, genuine and in her own words.
Here in this article she has wrote about the top 5 regrets that people have on their death bed. All of these are real, genuine and in her own words.
For many years I worked in palliative care. My patients were those who had gone home to die. Some incredibly special times were shared. I was with them for the last three to twelve weeks of their lives. People grow a lot when they are faced with their own mortality. I learnt never to underestimate someone’s capacity for growth. Some changes were phenomenal. Each experienced a variety of emotions, as expected, denial, fear, anger, remorse, more denial and eventually acceptance. Every single patient found their peace before they departed though, every one of them. When questioned about any regrets they had or anything they would do differently, common themes surfaced again and again. Here are the most common five: 1. I wish I’d had the courage to live a life true to myself, not the life others expected of me. This was the most common regret of all. When people realize that their life is almost over and look back clearly on it, it is easy to see how many dreams have gone unfulfilled. Most people had not honoured even a half of their dreams and had to die knowing that it was due to choices they had made, or not made. It is very important to try and honour at least some of your dreams along the way. From the moment that you lose your health, it is too late. Health brings a freedom very few realise, until they no longer have it. 2. I wish I didn’t work so hard. This came from every male patient that I nursed. They missed their children’s youth and their partner’s companionship. Women also spoke of this regret. But as most were from an older generation, many of the female patients had not been breadwinners. All of the men I nursed deeply regretted spending so much of their lives on the treadmill of a work existence. By simplifying your lifestyle and making conscious choices along the way, it is possible to not need the income that you think you do. And by creating more space in your life, you become happier and more open to new opportunities, ones more suited to your new lifestyle. 3. I wish I’d had the courage to express my feelings. Many people suppressed their feelings in order to keep peace with others. As a result, they settled for a mediocre existence and never became who they were truly capable of becoming. Many developed illnesses relating to the bitterness and resentment they carried as a result. We cannot control the reactions of others. However, although people may initially react when you change the way you are by speaking honestly, in the end it raises the relationship to a whole new and healthier level. Either that or it releases the unhealthy relationship from your life. Either way, you win. 4. I wish I had stayed in touch with my friends. Often they would not truly realise the full benefits of old friends until their dying weeks and it was not always possible to track them down. Many had become so caught up in their own lives that they had let golden friendships slip by over the years. There were many deep regrets about not giving friendships the time and effort that they deserved. Everyone misses their friends when they are dying. It is common for anyone in a busy lifestyle to let friendships slip. But when you are faced with your approaching death, the physical details of life fall away. People do want to get their financial affairs in order if possible. But it is not money or status that holds the true importance for them. They want to get things in order more for the benefit of those they love. Usually though, they are too ill and weary to ever manage this task. It is all comes down to love and relationships in the end. That is all that remains in the final weeks, love and relationships. 5. I wish that I had let myself be happier. This is a surprisingly common one. Many did not realise until the end that happiness is a choice. They had stayed stuck in old patterns and habits. The so-called ‘comfort’ of familiarity overflowed into their emotions, as well as their physical lives. Fear of change had them pretending to others, and to their selves, that they were content. When deep within, they longed to laugh properly and have silliness in their life again. When you are on your deathbed, what others think of you is a long way from your mind. How wonderful to be able to let go and smile again, long before you are dying.Life is a choice. It is YOUR life. Choose consciously, choose wisely, choose honestly. Choose happiness By Geeky Melanie – February 16, 2012Posted in: Bizarre- See more at: http://www.twosexygeeks.com/the-top-5-regrets-people-have-on-their-deathbed/#sthash.OR9MMmdx.dpuf
 Sexuality is a complex characteristic that involves the physical, psychological, interpersonal, and behavioral aspects of a person. Recognizing that "normal" sexual functioning covers a wide range is important. Ultimately, sexuality is defined by each patient and his/her partner according to sex, age, personal attitudes, and religious and cultural values.
Many types of cancer and cancer therapies can cause sexual dysfunction. Research shows that approximately 50% of women who have been treated for breast and gynecologic cancers experience long-term sexual dysfunction. Nearly 70% of men who have been treated for prostate cancer experience long-term sexual dysfunction.
An individual's sexual response can be affected in many ways. The causes of sexual dysfunction are often both physical and psychological. The most common sexual problems for people who have cancer are loss of desire for sexual activity in both men and women, problems achieving and maintaining an erection in men, and pain with intercourse in women. Men may also experience inability to ejaculate, ejaculation going backward into the bladder, or the inability to reach orgasm. Women may experience a change in genital sensations due to pain, loss of sensation and numbness, or decreased ability to reach orgasm. Most often, both men and women are still able to reach orgasm, however, it may be delayed due to medications and/or anxiety.
Unlike many other physical side effects of cancer treatment, sexual problems may not resolve within the first year or two of disease-free survival and can interfere with the return to a normal life. Patients recovering from cancer should discuss their concerns about sexual problems with a health care professional.
Factors Affecting Sexual Function in People With Cancer
Both physical and psychological factors contribute to the development of sexual dysfunction. Physical factors include loss of function due to the effects of cancer therapies, fatigue, and pain. Surgery, chemotherapy, and radiation therapy may have a direct physical impact on sexual function. Other factors that may contribute to sexual dysfunction include pain medications, depression, feelings of guilt from misbeliefs about the origin of the cancer, changes in body image after surgery, and stresses due to personal relationships. Getting older is often associated with a decrease in sexual desire and performance, however, sex may be important to the older person's quality of life and the loss of sexual function can be distressing.
Surgery-Related Factors
Surgery can directly affect sexual function. Factors that help predict a patient's sexual function after surgery include age, sexual and bladder function before surgery, tumor location and size, and how much tissue was removed during surgery. Surgeries that affect sexual function include breast cancer, colorectal cancer, prostate cancer, and other pelvic tumors.
Breast Cancer
Sexual function after breast cancer surgery has been the subject of much research. Surgery to save or reconstruct the breast appears to have little effect on sexual function compared with surgery to remove the whole breast. Women who have surgery to save the breast are more likely to continue to enjoy breast caressing, but there is no difference in areas such as how often women have sex, the ease of reaching orgasm, or overall sexual satisfaction.
Colorectal Cancer
Sexual and bladder dysfunctions are common complications of surgery for rectal cancer. The main cause of problems with erection, ejaculation, and orgasm is injury to nerves in the pelvic cavity. Nerves can be damaged when their blood supply is disrupted or when the nerves are cut.
Prostate Cancer
Newer nerve-sparing techniques for radical prostatectomy are being debated as a more successful approach for preserving erectile function than radiation therapy for prostate cancer. Long-term follow-up is needed to compare the effects of surgery with the effects of radiation therapy. Recovery of erectile function usually occurs within a year after having a radical prostatectomy. The effects of radiation therapy on erectile function are very slow and gradual occurring for two or three years after treatment. The cause of loss of erectile function differs between surgery and radiation therapy. Radical prostatectomy damages nerves that make blood vessels open wider to allow more blood into the penis. Eventually the tissue does not get enough oxygen, cells die, and scar tissue forms that interferes with erectile function. Radiation therapy appears to damage the arteries that bring blood to the penis.
Other Pelvic Tumors
Men who have surgery to remove the bladder, colon, and/or rectum may improve recovery of erectile function if nerve-sparing surgical techniques are used. The sexual side effects of radiation therapy for pelvic tumors are similar to those after prostate cancer treatment. Women who have surgery to remove the uterus, ovaries, bladder, or other organs in the abdomen or pelvis may experience pain and loss of sexual function depending on the amount of tissue/organ removed. With counseling and other medical treatments, these patients may regain normal sensation in the vagina and genital areas and be able to have pain-free intercourse and reach orgasm.
Chemotherapy-Related Factors
Chemotherapy is associated with a loss of desire and decreased frequency of intercourse for both men and women. The common side effects of chemotherapy such as nausea, vomiting, diarrhea, constipation, mucositis, weight loss or gain, and loss of hair can affect an individual's sexual self-image and make him or her feel unattractive.
For women, chemotherapy may cause vaginal dryness, pain with intercourse, and decreased ability to reach orgasm. In older women, chemotherapy may increase the risk of ovarian cancer. Chemotherapy may also cause a sudden loss of estrogen production from the ovaries. The loss of estrogen can cause shrinking, thinning, and loss of elasticity of the vagina, vaginal dryness, hot flashes, urinary tract infections, mood swings, fatigue, and irritability. Young women who have breast cancer and have had surgeries such as removal of one or both ovaries, may experience symptoms related to loss of estrogen. These women experience high rates of sexual problems since there is a concern that estrogen replacement therapy, which may decrease these symptoms, could cause the breast cancer to return. For women with other types of cancer, however, estrogen replacement therapy can usually resolve many sexual problems. Also, women who have graft-versus-host disease (a reaction of donated bone marrow or peripheral stem cells against a person's tissue) following bone marrow transplantation may develop scar tissue and narrowing of the vagina that can interfere with intercourse.
For men, sexual problems such as loss of desire and erectile dysfunction are more common after a bone marrow transplant because of graft-versus-host disease or nerve damage. Occasionally chemotherapy may interfere with testosterone production in the testicles. Testosterone replacement may be necessary to regain sexual function.
Radiation Therapy-Related Factors
Like chemotherapy, radiation therapy can cause side effects such as fatigue, nausea and vomiting, diarrhea, and other symptoms that can decrease feelings of sexuality. In women, radiation therapy to the pelvis can cause changes in the lining of the vagina. These changes eventually cause a narrowing of the vagina and formation of scar tissue that results in pain with intercourse, infertility and other long term sexual problems. Women should discuss concerns about these side effects with their doctor and ask about the use of a vaginal dilator.
For men, radiation therapy can cause problems with getting and keeping an erection. The exact cause of sexual problems after radiation therapy is unknown. Possible causes are nerve injury, a blockage of blood supply to the penis, or decreased levels of testosterone. Sexual changes occur very slowly over a period of six months to one year after radiation therapy. Men who had problems with erectile dysfunction before getting cancer have a greater risk of developing sexual problems after cancer diagnosis and treatment. Other risk factors that can contribute to a greater risk of sexual problems in men are cigarette smoking, history of heart disease, high blood pressure, and diabetes.
Hormone Therapy-Related Factors
Hormone therapy for prostate cancer can decrease normal hormone levels and cause a decrease in sexual desire, erectile dysfunction, and problems reaching orgasm. Younger men do not always experience the same degree of sexual dysfunction. Some treatment centers are experimenting with delayed or intermittent hormone therapy to prevent sexual problems. It is not yet known if these modified treatments affect the long-term survival of younger men.
The effects of tamoxifen on the sexuality and mood of women who have breast cancer are not clearly understood.
Psychological Factors
Patients recovering from cancer often have anxiety or guilt that previous sexual activities may have caused their cancer. Some patients believe that sexual activity may cause the cancer to return or pass the cancer to their partner. Discussing their feelings and concerns with a health care professional is important for patients. Misbeliefs can be corrected and patients can be reassured that cancer is not passed on through sexual contact.
Loss of sexual desire and a decrease in sexual pleasure are common symptoms of depression. Depression is more common in patients with cancer than in the general healthy population. It is important that patients discuss their feelings with their doctor. Getting treatment for depression may be helpful in relieving sexual problems.
Cancer treatments may cause physical changes that affect how an individual sees his or her physical appearance. This view can make a man or woman feel sexually unattractive. It is important that patients discuss these feelings and concerns with a health care professional. Patients can learn how to deal effectively with these problems.
The stress of being diagnosed with cancer and undergoing treatment for cancer can make existing problems in relationships even worse. The sexual relationship can also be affected. Patients who do not have a committed relationship may stop dating because they fear being rejected by a potential new partner who learns about their history of cancer. One of the most important factors in adjusting after cancer treatment is the patient's feeling about his or her sexuality before being diagnosed with cancer. If patients had positive feelings about sexuality, they may be more likely to resume sexual activity after treatment for cancer.
Assessment of Sexual Function in People with Cancer
Sexual function is an important factor that adds to quality of life. Patients should discuss their problems and concerns about sexual function with their doctor. Some doctors may not have the appropriate training to discuss sexual problems. Patients should ask for other information resources or for a referral to a health care professional who is comfortable with discussing sexuality issues.
General Factors Affecting Sexual Functioning
When a possible sexual problem is identified, the health care professional will do a detailed interview either with the patient alone or with the patient and his or her partner. The patient may be asked any of the following questions about his or her current and past sexual functioning:
Sexuality is a complex characteristic that involves the physical, psychological, interpersonal, and behavioral aspects of a person. Recognizing that "normal" sexual functioning covers a wide range is important. Ultimately, sexuality is defined by each patient and his/her partner according to sex, age, personal attitudes, and religious and cultural values.
Many types of cancer and cancer therapies can cause sexual dysfunction. Research shows that approximately 50% of women who have been treated for breast and gynecologic cancers experience long-term sexual dysfunction. Nearly 70% of men who have been treated for prostate cancer experience long-term sexual dysfunction.
An individual's sexual response can be affected in many ways. The causes of sexual dysfunction are often both physical and psychological. The most common sexual problems for people who have cancer are loss of desire for sexual activity in both men and women, problems achieving and maintaining an erection in men, and pain with intercourse in women. Men may also experience inability to ejaculate, ejaculation going backward into the bladder, or the inability to reach orgasm. Women may experience a change in genital sensations due to pain, loss of sensation and numbness, or decreased ability to reach orgasm. Most often, both men and women are still able to reach orgasm, however, it may be delayed due to medications and/or anxiety.
Unlike many other physical side effects of cancer treatment, sexual problems may not resolve within the first year or two of disease-free survival and can interfere with the return to a normal life. Patients recovering from cancer should discuss their concerns about sexual problems with a health care professional.
Factors Affecting Sexual Function in People With Cancer
Both physical and psychological factors contribute to the development of sexual dysfunction. Physical factors include loss of function due to the effects of cancer therapies, fatigue, and pain. Surgery, chemotherapy, and radiation therapy may have a direct physical impact on sexual function. Other factors that may contribute to sexual dysfunction include pain medications, depression, feelings of guilt from misbeliefs about the origin of the cancer, changes in body image after surgery, and stresses due to personal relationships. Getting older is often associated with a decrease in sexual desire and performance, however, sex may be important to the older person's quality of life and the loss of sexual function can be distressing.
Surgery-Related Factors
Surgery can directly affect sexual function. Factors that help predict a patient's sexual function after surgery include age, sexual and bladder function before surgery, tumor location and size, and how much tissue was removed during surgery. Surgeries that affect sexual function include breast cancer, colorectal cancer, prostate cancer, and other pelvic tumors.
Breast Cancer
Sexual function after breast cancer surgery has been the subject of much research. Surgery to save or reconstruct the breast appears to have little effect on sexual function compared with surgery to remove the whole breast. Women who have surgery to save the breast are more likely to continue to enjoy breast caressing, but there is no difference in areas such as how often women have sex, the ease of reaching orgasm, or overall sexual satisfaction.
Colorectal Cancer
Sexual and bladder dysfunctions are common complications of surgery for rectal cancer. The main cause of problems with erection, ejaculation, and orgasm is injury to nerves in the pelvic cavity. Nerves can be damaged when their blood supply is disrupted or when the nerves are cut.
Prostate Cancer
Newer nerve-sparing techniques for radical prostatectomy are being debated as a more successful approach for preserving erectile function than radiation therapy for prostate cancer. Long-term follow-up is needed to compare the effects of surgery with the effects of radiation therapy. Recovery of erectile function usually occurs within a year after having a radical prostatectomy. The effects of radiation therapy on erectile function are very slow and gradual occurring for two or three years after treatment. The cause of loss of erectile function differs between surgery and radiation therapy. Radical prostatectomy damages nerves that make blood vessels open wider to allow more blood into the penis. Eventually the tissue does not get enough oxygen, cells die, and scar tissue forms that interferes with erectile function. Radiation therapy appears to damage the arteries that bring blood to the penis.
Other Pelvic Tumors
Men who have surgery to remove the bladder, colon, and/or rectum may improve recovery of erectile function if nerve-sparing surgical techniques are used. The sexual side effects of radiation therapy for pelvic tumors are similar to those after prostate cancer treatment. Women who have surgery to remove the uterus, ovaries, bladder, or other organs in the abdomen or pelvis may experience pain and loss of sexual function depending on the amount of tissue/organ removed. With counseling and other medical treatments, these patients may regain normal sensation in the vagina and genital areas and be able to have pain-free intercourse and reach orgasm.
Chemotherapy-Related Factors
Chemotherapy is associated with a loss of desire and decreased frequency of intercourse for both men and women. The common side effects of chemotherapy such as nausea, vomiting, diarrhea, constipation, mucositis, weight loss or gain, and loss of hair can affect an individual's sexual self-image and make him or her feel unattractive.
For women, chemotherapy may cause vaginal dryness, pain with intercourse, and decreased ability to reach orgasm. In older women, chemotherapy may increase the risk of ovarian cancer. Chemotherapy may also cause a sudden loss of estrogen production from the ovaries. The loss of estrogen can cause shrinking, thinning, and loss of elasticity of the vagina, vaginal dryness, hot flashes, urinary tract infections, mood swings, fatigue, and irritability. Young women who have breast cancer and have had surgeries such as removal of one or both ovaries, may experience symptoms related to loss of estrogen. These women experience high rates of sexual problems since there is a concern that estrogen replacement therapy, which may decrease these symptoms, could cause the breast cancer to return. For women with other types of cancer, however, estrogen replacement therapy can usually resolve many sexual problems. Also, women who have graft-versus-host disease (a reaction of donated bone marrow or peripheral stem cells against a person's tissue) following bone marrow transplantation may develop scar tissue and narrowing of the vagina that can interfere with intercourse.
For men, sexual problems such as loss of desire and erectile dysfunction are more common after a bone marrow transplant because of graft-versus-host disease or nerve damage. Occasionally chemotherapy may interfere with testosterone production in the testicles. Testosterone replacement may be necessary to regain sexual function.
Radiation Therapy-Related Factors
Like chemotherapy, radiation therapy can cause side effects such as fatigue, nausea and vomiting, diarrhea, and other symptoms that can decrease feelings of sexuality. In women, radiation therapy to the pelvis can cause changes in the lining of the vagina. These changes eventually cause a narrowing of the vagina and formation of scar tissue that results in pain with intercourse, infertility and other long term sexual problems. Women should discuss concerns about these side effects with their doctor and ask about the use of a vaginal dilator.
For men, radiation therapy can cause problems with getting and keeping an erection. The exact cause of sexual problems after radiation therapy is unknown. Possible causes are nerve injury, a blockage of blood supply to the penis, or decreased levels of testosterone. Sexual changes occur very slowly over a period of six months to one year after radiation therapy. Men who had problems with erectile dysfunction before getting cancer have a greater risk of developing sexual problems after cancer diagnosis and treatment. Other risk factors that can contribute to a greater risk of sexual problems in men are cigarette smoking, history of heart disease, high blood pressure, and diabetes.
Hormone Therapy-Related Factors
Hormone therapy for prostate cancer can decrease normal hormone levels and cause a decrease in sexual desire, erectile dysfunction, and problems reaching orgasm. Younger men do not always experience the same degree of sexual dysfunction. Some treatment centers are experimenting with delayed or intermittent hormone therapy to prevent sexual problems. It is not yet known if these modified treatments affect the long-term survival of younger men.
The effects of tamoxifen on the sexuality and mood of women who have breast cancer are not clearly understood.
Psychological Factors
Patients recovering from cancer often have anxiety or guilt that previous sexual activities may have caused their cancer. Some patients believe that sexual activity may cause the cancer to return or pass the cancer to their partner. Discussing their feelings and concerns with a health care professional is important for patients. Misbeliefs can be corrected and patients can be reassured that cancer is not passed on through sexual contact.
Loss of sexual desire and a decrease in sexual pleasure are common symptoms of depression. Depression is more common in patients with cancer than in the general healthy population. It is important that patients discuss their feelings with their doctor. Getting treatment for depression may be helpful in relieving sexual problems.
Cancer treatments may cause physical changes that affect how an individual sees his or her physical appearance. This view can make a man or woman feel sexually unattractive. It is important that patients discuss these feelings and concerns with a health care professional. Patients can learn how to deal effectively with these problems.
The stress of being diagnosed with cancer and undergoing treatment for cancer can make existing problems in relationships even worse. The sexual relationship can also be affected. Patients who do not have a committed relationship may stop dating because they fear being rejected by a potential new partner who learns about their history of cancer. One of the most important factors in adjusting after cancer treatment is the patient's feeling about his or her sexuality before being diagnosed with cancer. If patients had positive feelings about sexuality, they may be more likely to resume sexual activity after treatment for cancer.
Assessment of Sexual Function in People with Cancer
Sexual function is an important factor that adds to quality of life. Patients should discuss their problems and concerns about sexual function with their doctor. Some doctors may not have the appropriate training to discuss sexual problems. Patients should ask for other information resources or for a referral to a health care professional who is comfortable with discussing sexuality issues.
General Factors Affecting Sexual Functioning
When a possible sexual problem is identified, the health care professional will do a detailed interview either with the patient alone or with the patient and his or her partner. The patient may be asked any of the following questions about his or her current and past sexual functioning:
The human body is complex and beautiful. It gives you pleasure and pain, and it is both strong and fragile. While we all come into this world wearing nothing, nudity is one of the strongest taboos that have ever existed in our society. We cover and protect our own bodies, but do we really cherish them?
Nude yoga is a form of yoga practice that accentuates the perfection of the human body. It teaches to understand, appreciate, and cherish your physique. It’s the simplest and most natural way to start a healthier and happier life by learning the techniques of gentle workout and meditation.
Nude yoga isn’t mainstream and it really isn’t for everyone, but it can turn you into an artist who rediscovers and rebuilds his body beautiful.
http://youtu.be/Tv73udbijmY source: http://nudeyoga.org.uk/ Post by: HeatherB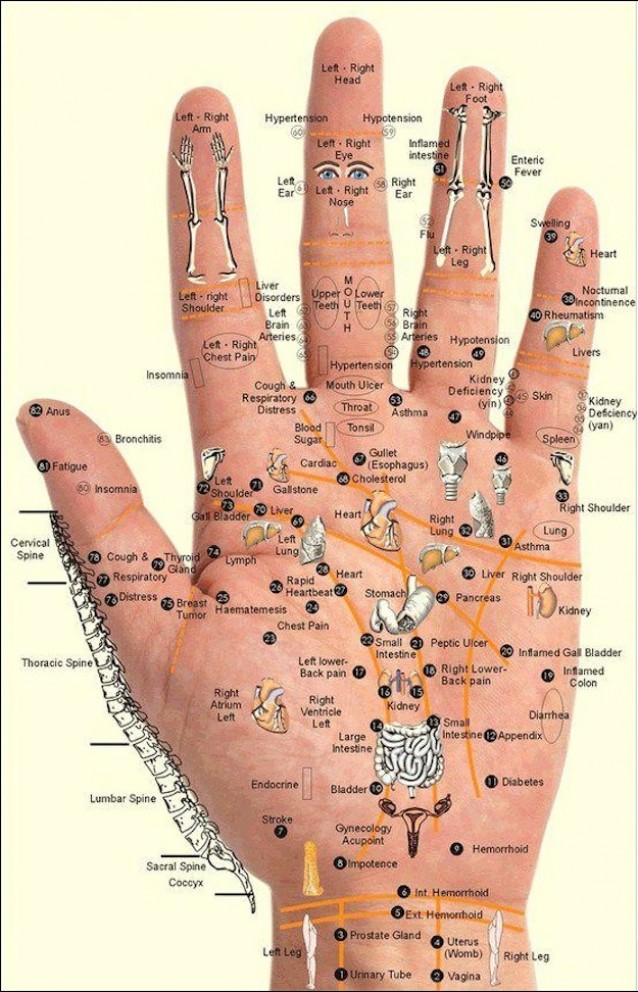 This Chart and Techniques for Hand Reflexology and Massage of Meridian points shows us where and how to use our own personal power and take charge of our health.
This Chart and Techniques for Hand Reflexology and Massage of Meridian points shows us where and how to use our own personal power and take charge of our health.
 The Federal Government is making their place clear (er). We are happy to read the following document released just today:
http://www.justice.gov/iso/opa/resources/3052013829132756857467.pdf
Our favorite line:
The Federal Government is making their place clear (er). We are happy to read the following document released just today:
http://www.justice.gov/iso/opa/resources/3052013829132756857467.pdf
Our favorite line:
 YEAH, YOU LIKELY MISUSED FEDERAL RESOURCES....just like we've yelled for decades now. END PROHIBITION.
YEAH, YOU LIKELY MISUSED FEDERAL RESOURCES....just like we've yelled for decades now. END PROHIBITION.
 Our heart goes out to all of our family members, friends and all beings who have been adversely effected by the misuse of the powers that be. Think of all the patients who needed this medicine, would've been cured, found comfort in the worst of times and appetite when going through the thick of it.
So many states have legalized....yet there are many more that need to get with the program. Ahem, Texas. (the place of Ganja Vibe's inception)
This fight will continue and if the truth shall set you free, then as GOD as my witness.....We Will Win!
Skeptics take note. To the commercial public, the freedom fighters in our nation, who are ballsy enough to come out of the underground, are walking on water. We need you to WAKE UP.
Other related links:
http://www.washingtonpost.com/national/health-science/obama-administration-will-not-preempt-state-marijuana-laws--for-now/2013/08/29/b725bfd8-10bd-11e3-8cdd-bcdc09410972_story.html?wpisrc=al_comboPN
http://www.usatoday.com/story/news/nation/2013/08/29/justice-medical-marijuana-laws/2727605/
~ HeatherB
Our heart goes out to all of our family members, friends and all beings who have been adversely effected by the misuse of the powers that be. Think of all the patients who needed this medicine, would've been cured, found comfort in the worst of times and appetite when going through the thick of it.
So many states have legalized....yet there are many more that need to get with the program. Ahem, Texas. (the place of Ganja Vibe's inception)
This fight will continue and if the truth shall set you free, then as GOD as my witness.....We Will Win!
Skeptics take note. To the commercial public, the freedom fighters in our nation, who are ballsy enough to come out of the underground, are walking on water. We need you to WAKE UP.
Other related links:
http://www.washingtonpost.com/national/health-science/obama-administration-will-not-preempt-state-marijuana-laws--for-now/2013/08/29/b725bfd8-10bd-11e3-8cdd-bcdc09410972_story.html?wpisrc=al_comboPN
http://www.usatoday.com/story/news/nation/2013/08/29/justice-medical-marijuana-laws/2727605/
~ HeatherB
Subscribe to our newsletter and always be the first to hear about what is happening.
© 2026 Ganja Vibes. This website is for 18+ and contains adult content.